

Theme
9BB Simulation 1
INSTITUTION
Office of Medical Education - Tohoku University Graduate School of Medicine - Sendai - Japan
Graduate Medical Education Center - Tohoku University Hospital - Sendai - Japan

Medical students should acquire the competency of cardiac auscultation before initiating clinical clerkship. Although simulators are useful for the students to learn a variety of medical skills, efficacy of high-fidelity simulators in cardiac-auscultation training is still controversial.1-5
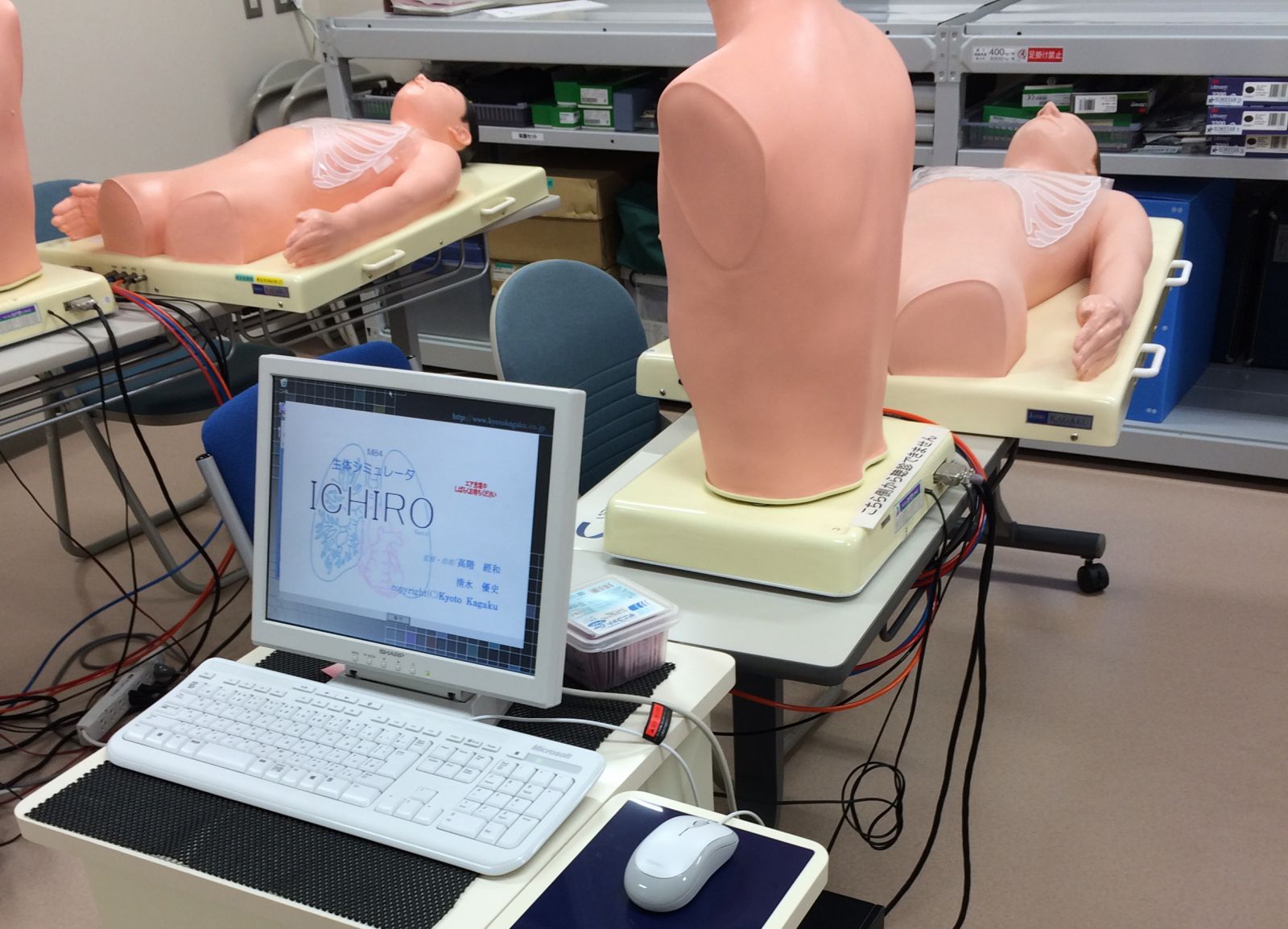
A total of 324 fourth-year medical students (93-117/year for 3 years) were divided into groups of 7-8 students, and participated in 3-hour cardiac-auscultation training using patient simulators (“K”, Kyoto Kagaku). After a mini-lecture and facilitated training, the students took two different tests using the simulators.
Figure 1. Simulator "K" ("Ichiro" in Japan) and Mr. Lung
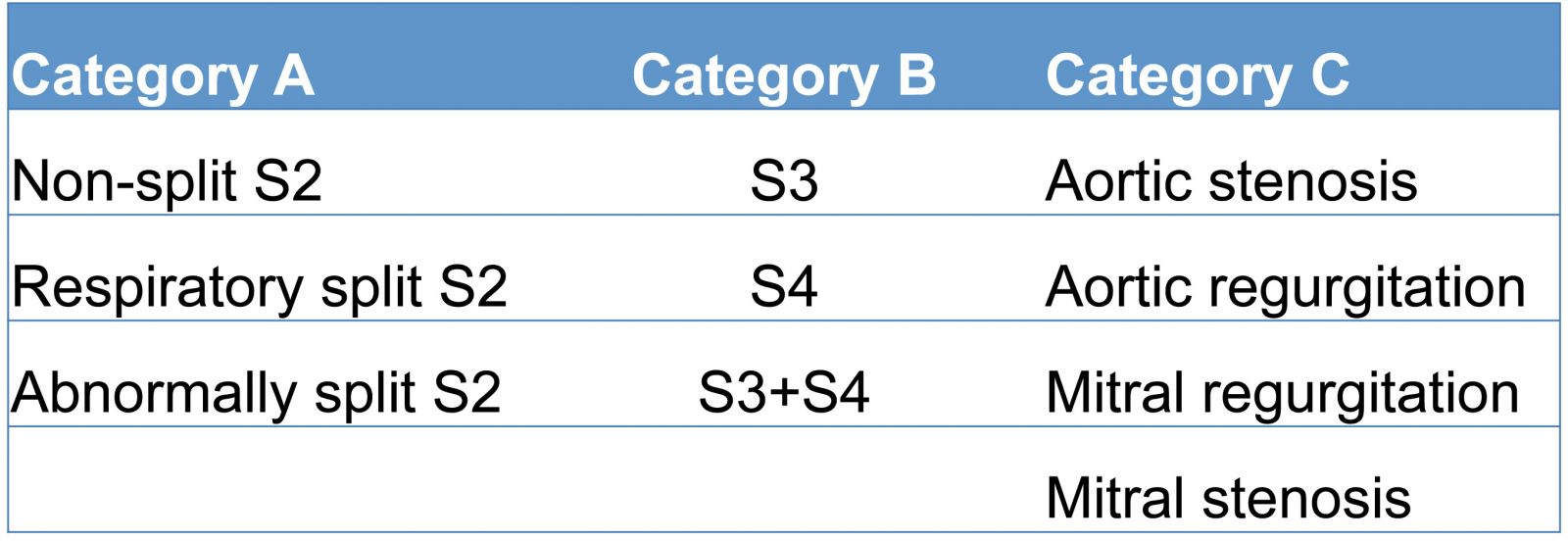
In the first test, they listened to three sounds of Category A (non-split S2, respiratory split S2 and abnormally split S2) in random order, but being informed that those three were from Category A, and identified each sound. The students answered in the same way regarding Category B (S3, S4 and S3+S4) and Category C (aortic stenosis, aortic regurgitation, mitral regurgitation and mitral stenosis).
In the second test, the students listened to only one from each of the three categories in random order without any category information, and identified each.
Table 1. Three categories of heart sounds
Ethical approval was obtained from the Ethical Committee of Tohoku University Graduate School of Medicine (Protocol number 2013-1-210).
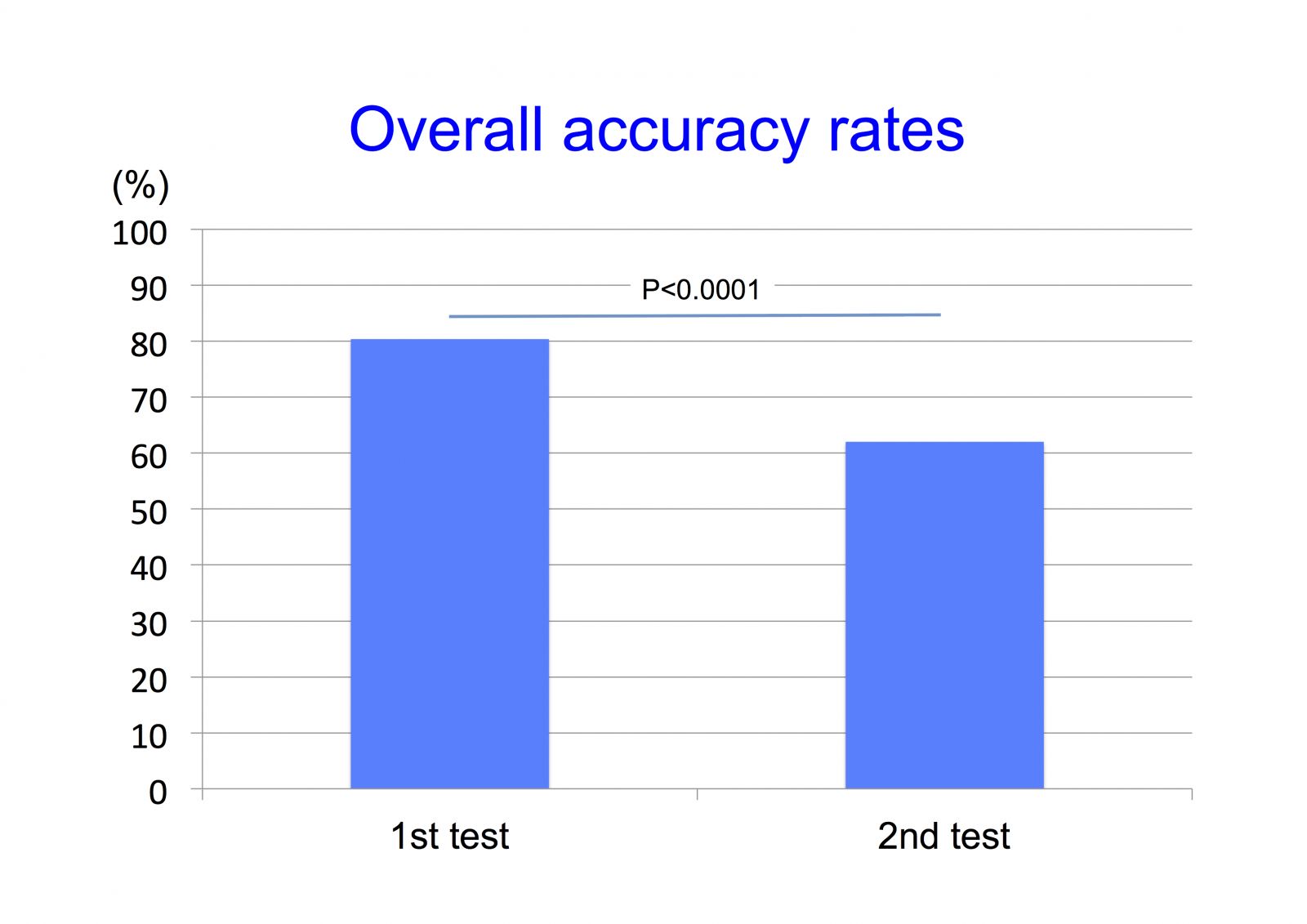
The overall accuracy rate was 80% in the first test and 62% in the second test (P<0.0001).
Figure 1. Overall accuracy rates in the two difenrent types of tests in the cardiac-auscultation training class
In the first test, the accuracy rates were 87%, 86%, 93% for each sound of Category A, 73%, 73%, 67% for each of Category B, and 89%, 81%, 78%, 77% for each of Category C, respectively (n=324 for each).
In the second test, the accuracy rates were 51%*, 59%*, 60%* for Category A, 49%*, 65%, 42%* for Category B, and 95%, 71%, 78%, 67% for Category C, respectively (*P<0.0001 vs. the first test, n=77-114 for each).
Figure 2. Accuracy rates in the two different types of tests
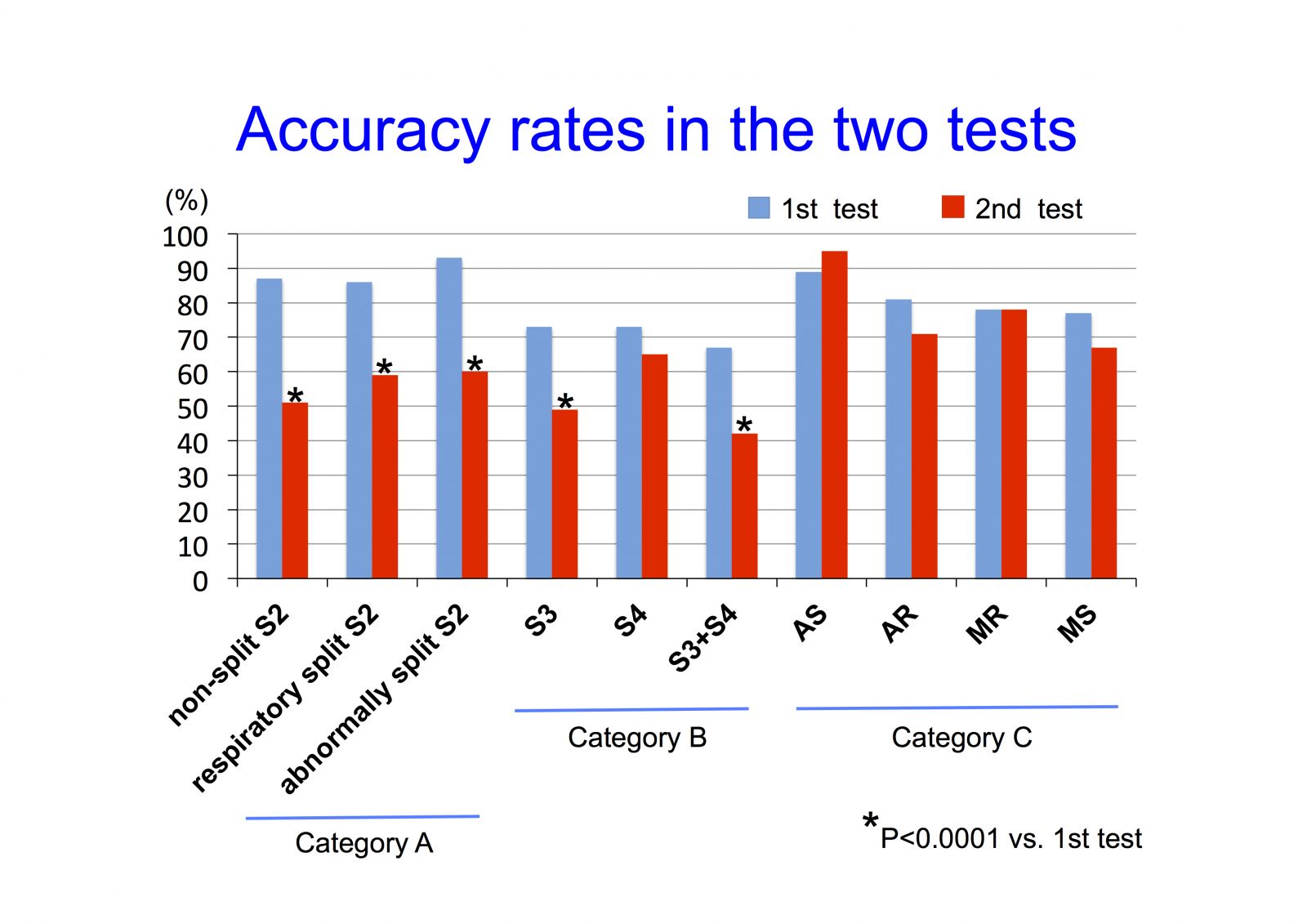
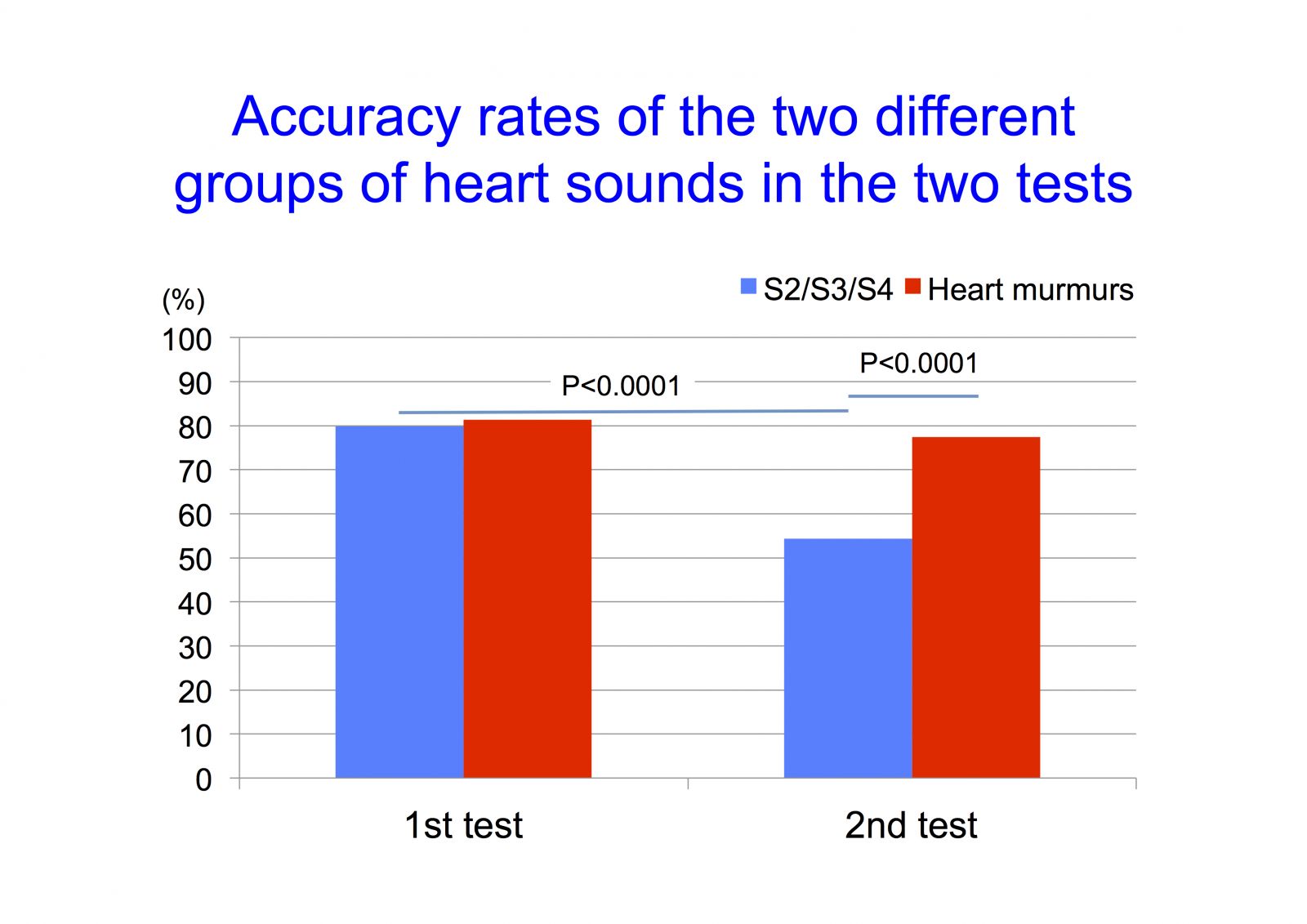
Figure 3. Accuracy rates of the two different groups of heart sounds in the two tests
1. The accuracy rates were lower in the second test, which was closer to clinical setting than the first test. The medical students were less likely to correctly identify heart sounds when they were not informed of the categories of heart sounds.
2. The students were less likely to correctly identify S2/S3/S4 than heart murmurs in the second test, but not in the first test.
This study was supported in part by Grants-in-Aid for Science Research (25460608) from the Ministry of Education, Culture, Sports and Technology in Japan.
A single cardiac-auscultation training class using a high-fidelity simulator alone may not be sufficient to achieve competence necessary for clinical clerkship.
1. Butter J, McGaghie WC, Cohen ER, Kaye M, Wayne DB. Simulation-based mastery learning improves cardiac auscultation skills in medical students. J Gen Intern Med. 2010;25:780-5.
2. Chen R, Grierson LE, Norman GR. Evaluating the impact of high- and low-fidelity instruction in the development of auscultation skills. Med Educ. 2015;49:276-85.
3. de Giovanni D, Roberts T, Norman G. Relative effectiveness of high- versus low-fidelity simulation in learning heart sounds. Med Educ. 2009;43:661-8.
4. Fraser K, Wright B, Girard L, Tworek J, Paget M, Welikovich L, McLaughlin K. Simulation training improves diagnostic performance on a real patient with similar clinical findings. Chest. 2011;139:376-81.
5. McKinney J, Cook DA, Wood D, Hatala R. Simulation-based training for cardiac auscultation skills: systematic review and meta-analysis. J Gen Intern Med. 2013;28:283-91.
 Send Email
Send Email