
| Theme: Postgraduate Education | |||
 |
||||||
| Residents' Perspective of New Accreditation Council for Graduate Medical Education Ophthalmology Program in Singapore |
 |
|||||
|
||||||

Graduate medical education in Singapore has long been overseen by surgeons and physicians appointed to the Joint Committee on Specialist Training (JCST). The JCST served to select trainees, establish and maintain structured training programs and accredit training places. Most programs were modelled after British training programs. In recent years, Singapore has looked to adopting the American graduate medical education system and hence implemented the programs of the Accreditation Council for Graduate Medical Education (ACGME). Since 2010, healthcare institutions across Singapore have adopted the ACGME programs for new trainees. The Department of Ophthalmology at the National Healthcare group now runs both systems concurrently with pre-existing trainees continuing on the original track and new trainees starting on the ACGME program.
Having had the ACGME Ophthalmology program run alongside the department’s original training program for more than a year, we would like to assess how residents feel about the program and the quality of training within the department. We would like to gain an understanding into the perceived pros and cons of the new training program and how it may be better adapted to suit the needs of local trainees.
A survey was carried out amongst all residents in the National Healthcare Group Ophthalmology Program.
The survey looked into 4 core areas of the training program. Program induction, clinical and educational supervision, institutional and departmental educational programs and working hours. A total of 8 residents in the program were given a copy of the survey, with a response rate of 100%. Of the 8 residents, 4 were in Year 1 and 4 in Year 2 of the Ophthalmology program.
All residents reported that their roles and responsibilities were explained to them at the commencement of their training and each of them keeps a learning portfolio and logbook.
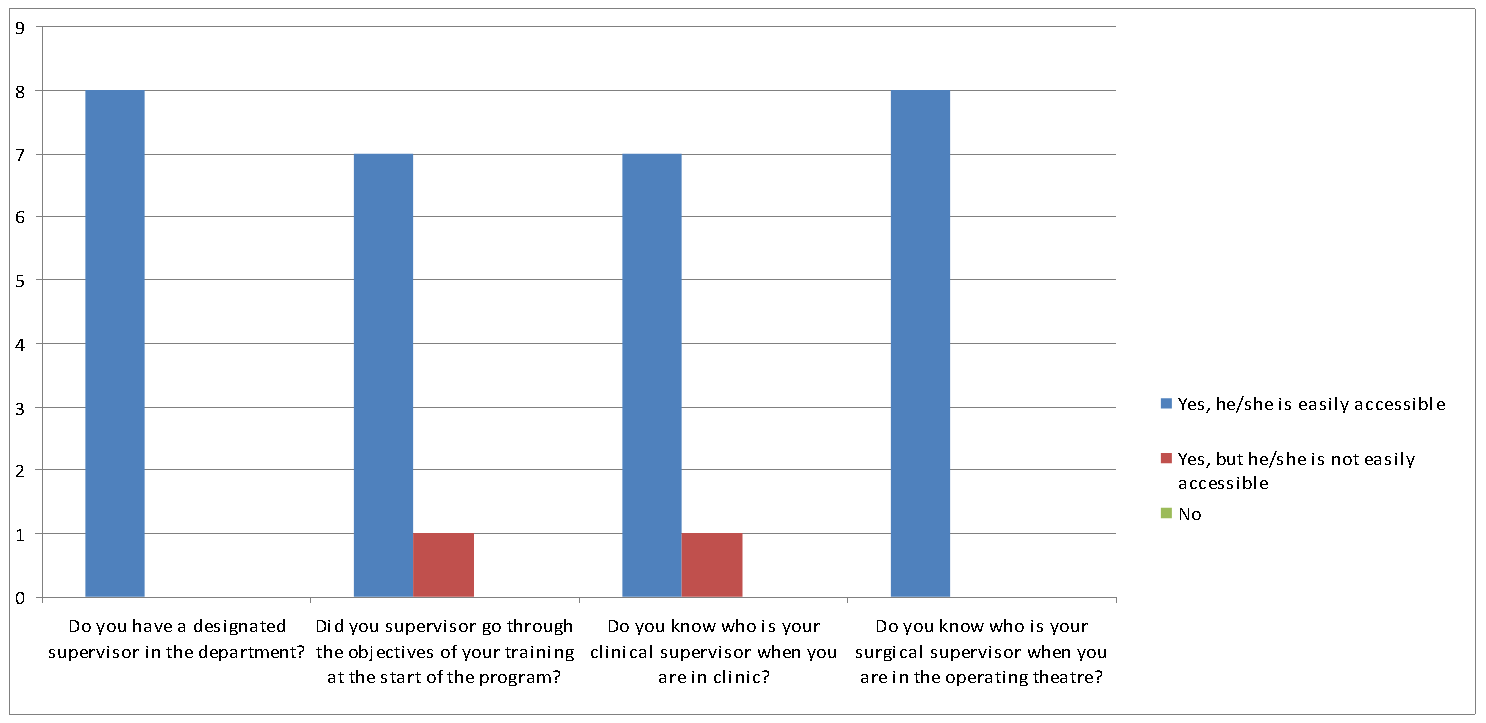
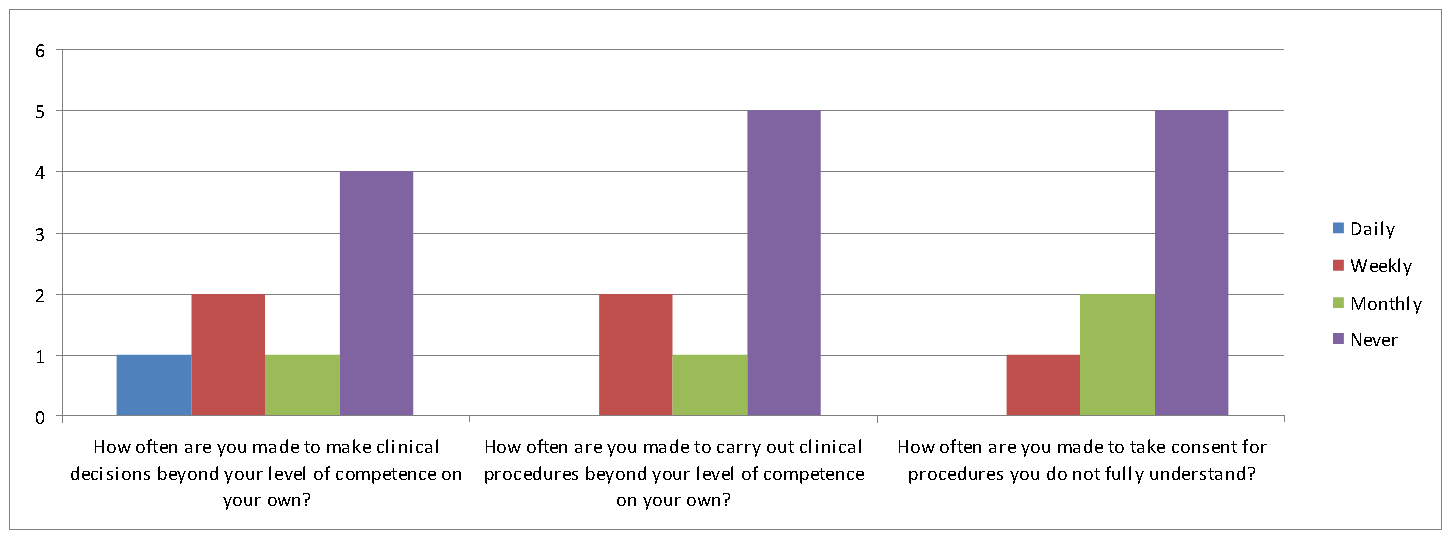
Clinical and educational supervision
With respect to clinical supervision within the department, more than half of the residents reported they were never made to make clinical decisions or carry out clinical procedures beyond their level independently. All residents were acquainted with their educational supervisors and reported they were easily accessible.
Institutional and Departmental Educational Program
All residents felt that the department’s clinical case load provided a sufficient breadth and depth for their learning but 2 of 8 (25%) felt that there were insufficient opportunities to assist in surgical procedures. 7 of 8 (87.5%) of residents reported that the department adhered to a systematic teaching schedule and all residents found the sessions clinically relevant. With respect to attendance of core courses organised by the Sponsoring Institution, only 3 of 8 (37.5%) found the subject matter appropriate and only 2 of 8 (25%) found the sessions clinically relevant.
Working Hours
None of the residents reported a violation of duty hours but 1 resident (12.5%) felt that the strict ACGME duty hours curtailed learning opportunities.
Half the residents felt the shortened training period could put them at a disadvantage at times but 5 of 8 (62.5%) rated the new training program as being better than the original training program. On a scale from 1-5 regarding confidence of being able to work independently upon completion of the program, the mean score of all residents was 3.69 and the mode 4.
Survey findings suggest a structured and well organised program in place with compliance to ACGME requirements of duty hours and attendance of institutional core courses.
In keeping with the competency based program, residents cited the rigorous syllabus and multiple formative assessments as the main reasons they found the new program better.
Residents who found the program no better than the original training program explained that the department already had in place its own teaching schedule and formative assessments and cited the extensive administrative work in the new program as its main downside.
The new ACGME program provides a streamlined yet rigorous training schedule. Whilst the training period has been shortened, residents are confident that they will be equipped with the skills to work independently upon completion of the program.
Philbert I, Satisfiers and
Hygiene Factors: Residents’ Perceptions of Strengths and Limitations of Their Learning Environment, J Grad Med Educ., 2012 March; 4(1):122-127
Lee AG, Oetting T, Beaver HA, Carter K, Task Force on the ACGME Competencies at the University of Iowa Department of Ophthalmology, The ACGME Outcome Project in ophthalmology: Practical recommendations for overcoming the barriers to local implementation of the national mandate.,
Surv Ophthalmol, 2009 Jul-Aug; 54(4):507-17
 Send Email
Send Email