 Send Email
Send Email

|
Authors | Institution |
|
Lorenzo Tagliabue Deborah Corrias Giorgio Rezzonico Maria Grazia Strepparava |
Milano Bicocca University, School of Medicine San Gerardo Hospital, Monza |
 |
|
||||||
| Personality differences in communication skills and attitudes in a sample of Italian medical students |

The shift from the “disease-centered” approach to the “patient-centered” attitude in medicine lead to an increasing attention to communication skills in the medical training and to the relational aspects involved in the medical encounter. The ability to well conduct a clinical inquiry is not any more believed to be only an inborn skill (Mead and Bower, 2000) and many researches have been done in the last decade to identify the core issues and the best strategies for achiving a real patient-oriented attitude in Medical Doctor (e.g. narrative medicine, problem based learning and so on). A lot of work was done also on the role of physician empathy in patient care (see Hojat, 2007), but there are many aspect of individual functioning relevant to communication and interaction that are still underexplored.
Aim of this research is to study the performance during a role-play in a sample of MD students, linking their communicative style to personality differences.
SAMPLE: 21 third, fourth and fifth year students (14 females, 7 males) with at least one year of hospital ward experience
PROCEDURE: Each student acted as doctor in a standardized role-playing (cancer diagnosis communication), with a standardized patient (played by a skilled psychologist) and filled in a set of questionnaires for personality profiling.
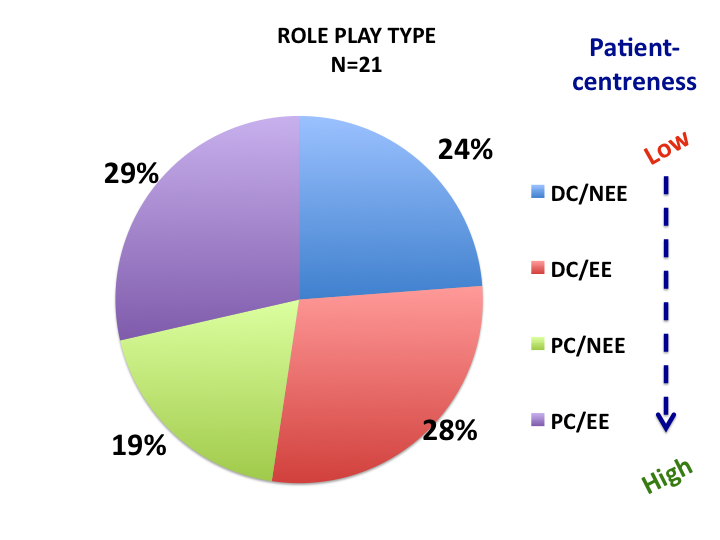
VIDEO ANALYSIS: The 21 role-plays (mean duration = 14, 65 min) were videotaped and transcript were analyzed by (1) the Roter Interaction Analysis System (Roter, Larson, 2002) and (2) the Verona Network on Sequences Analysis VNSA (Del Piccolo et al 2011). Combining the “task focused” (or problem solving behaviour) and the “socio-emotional” (or affective behaviour) categories of RIAS (see Mead and Bower 2000) with the “emotional exploration “ and “no emotional exploration" of VNSA, video-transcripts were classified in four groups, according to the patient-centredness level, ranging from the less patient-centred - Disease-Centred with No Emotional Exploration DC/NEE; Disease-Centred with Emotional Exploration DC/EE - to the more patient-centred - Patient-Centred with No Emotional Exploration PC/NEE; Patient-Centred with Emotional Exploration PC/EE.
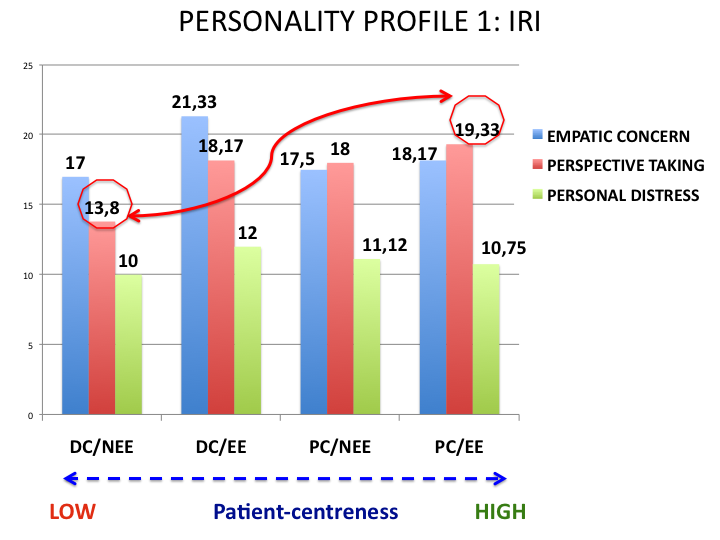
PERSONALITY ASSESSMENT: Personality profiles were assessed by: Interpersonal Reactivity Index (Davis, 1983), Self Monitoring Scale (Snyder, 1974), Patient Practioner Orientation Scale (Krupat, 2004), and a subset of items of the Personal Meaning Questionnaire QSP, Personality Scale (Picardi et al. 2003).
An intergroup comparison of the personality profiles of MD students was conducted; role-play classification (DC/NEE, DC/EE, PC/NEE, PC/EE) was used as grouping vatiable
.png)
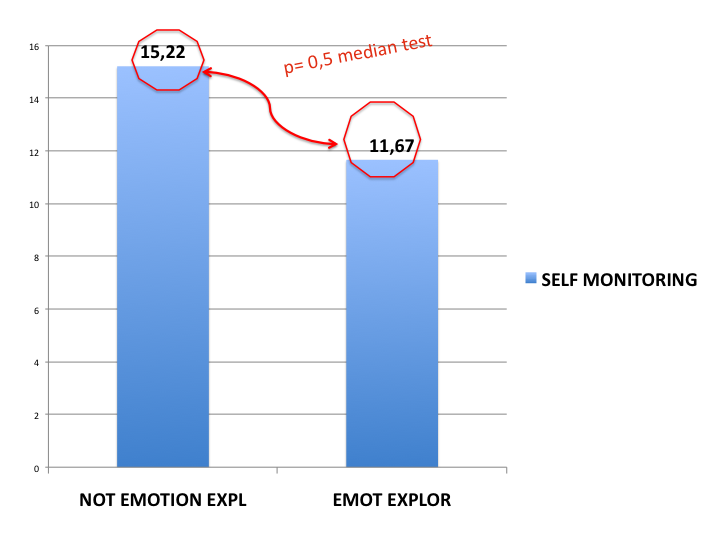
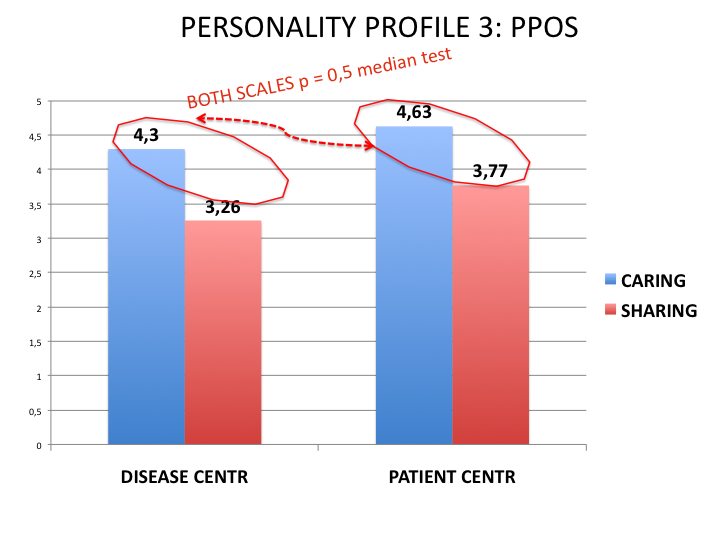
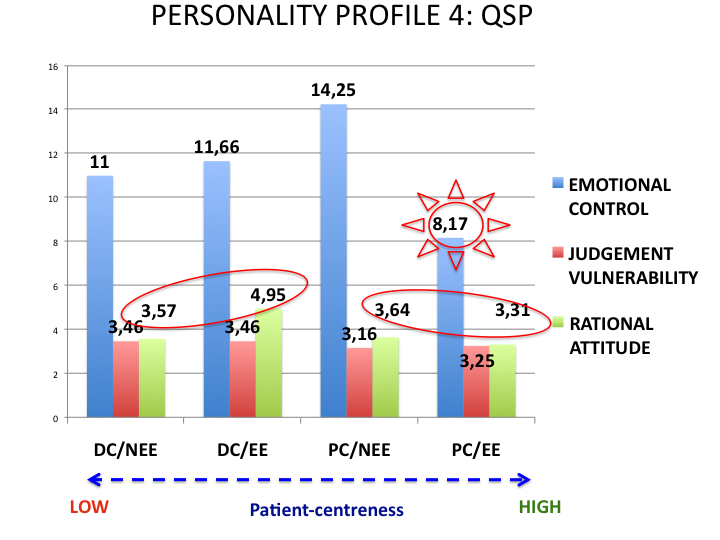
A different performance in the role-play situation is connected with differences in some dimensions of the personality profile: MD students who display a more patient-centred behaviour (e.g. showing concern, verbal attentiveness, kindness, sensibility to and exploration of patient’s emotions) are more skilled in perspective taking, less vulnerable to personal distress in critical situation, slightly more sensible to the caring and sharing issues in patient-doctor communication, less prone to be detached during the interaction and have a lower need to control their own emotions during the medical talk. As last, the tendency to display true dispositions and attitudes in every situations seems to help the MD student in exploring patient’s emotions during the medical consultation.
First: there are differences in personality profile of MD-students with different communication style (patient vrs disease oriented) as measured by objective and subjective measures (trascript analysis and self-report questionnaire)
Second: nevertheless the link between personality and performance is not simple, direct or clear and the variables interaction need to be more deeply understood
Third: one help to adequately develop this kind of research is to conduct longitudinal studies to better identify what are stable personality traits and what can be modified by the training interventions with a test-retest procedure
Davis, Mark H. (1983) Measuring individual differences in empathy: Evidence for a multidimensional approach. Journal of Personality and Social Psychology, Vol 44(1), 113-126
Krupat E., Hsu J., Schmittdiel j.A., Selby J., (2004). “Matching patients and practitioners based on belief about care: results of a randomized controlled trilal”. American Journalof Managed Care. 10, 814-822.
Hojat M. (2007). “Empathy in patient care”. Springer NY
Mead N., Bower P., (2000). “Patient centredness: a conceptual framework and review of the empirical literature”. Social Science and Medicine. 51, 1087-1100
Picardi A., Mannino G., Arciero G., Gaetano P., Pilleri M.F., Arduini L., Vistarini L., Reda M.A., (2003). “Costruzione e validazione del QSP, uno strumento per la valutazione dello stile di personalità secondo la teoria delle “organizzazioni di significato personale”. Rivista di Psichiatria. 38; 13-34.
Piccolo, L. del, Haes, H. de, Heaven, C., Jansen, J., et al. (2011). Development of the Verona coding definitions of emotional sequences to code health providers' responses (VR-CoDES-P) to patient cues and concerns. Patient Education and Counseling, 82(2), 149-155
Roter D., Larson S., (2002). “The roter interaction analysis system (RIAS): utility and flexibility for analysis of medical interactions”. Patient Educational Counselling. 46, 243-252
Snyder M., (1974). “Self Monitoring of expressive behavior.” Journal of Personality and Social Psychology. 30, 526-537
This work was supported by grants from the Italian Ministry of University
and Research: FAR 2010-2011 (ex 60 %)